I understand the LMRFD has a new automatic CPR machine. This will give patients who suffer a heart attack or sudden cardiac arrest and require CPR a chance at life.
These CPR machines do very effective CPR at the correct depth and rate and they don't get tired.
I understand the new CPR machine will be in Meadview. I would have hoped they would have it on the ambulance rather than in Meadview.
Now that cardiac patients have a chance of survival we need to teach CPR and AED use to everyone and anyone who is willing to learn, for free...
I don't care if they get a CPR card. You don't need a card to do CPR, you just need to do it in an effective manner if you want the patient to have a chance of survival.
Friday, December 7, 2018
Friday, November 2, 2018
2018 Northern Arizona Consolidated Fire District #1 (NACFD1) Board of Directors Election - Who to Vote For
2018 Northern
Arizona Consolidated Fire District #1 (NACFD1)
Board of
Directors Election - Who to Vote For
This
year's election for two vacant seats on the board is critical to saving our
fire district. Candidates Gerald Lucero and Sue Wilkin are the only choices for
the board. The district is currently operating with illegally appointed
directors, Erik Berg and candidate John Bryant. These Directors were appointed
illegally by Chairman Jim Bailey and Clerk Mike Collins and have no business
serving on our board. Since their appointment, Bailey and Collins are trying to
cover their tracks after spearheading an effort to waste public funds by
purchasing a former feed store for $500,000 in 2012 for use as a fire station.
Over six years later, the building sits without an occupancy permit and no work
has been completed. They need their cronies to help clean up this mess.
Ironically, John Bryant had never attended a board meeting and showed up
mysteriously to be appointed to a vacancy as Bailey and Collins spun a web of
lies to chase off three directors and illegally terminate the fire chief and
administrative assistant. John Bryant has no clue of what to do as a director.
Gerald
Lucero, formally served as a Battalion Chief for the Valle Vista and Hualapai
valley Fire Districts. He has a strong background in public administration
thanks to his service as a Federal employee. Sue Wilkin formally served on the
NACFD1 Board of Directors until Bailey and Collins filed false statements with
the Mohave County Attorney's Office. She has now been cleared and once again
may serve on the Board. She has previously served on the Citizen's Support
Group for the Hualapai Valley Fire District; various committees for NACFD1; and
currently serves on NACFD1's Retirement Board. Bailey and Collins will do
everything they can to stop Lucero and Wilkin from being elected. Don't fall
into their trap. Vote for Gerald Lucero and Sue Wilkin for the NACFD1 Board.
Help stop the lies and multiple claims filed against the district in the last
several months.
Wednesday, October 24, 2018
Life and Death in Dolan Springs the Lake Mohave Ranchos Fire District just passed 22,000 views
Last week the Life and Death in Dolan Springs the Lake Mohave Ranchos Fire District Blog just passed 22,000 views from all over the world....
Monday, October 8, 2018
Questions We Need to Ask..... Fire Board Candidates
The LMRFD Ambulance that covers over 2000sm's is only supported by the taxpayers of the 144sm fire district.
The ambulance needs to be run like a business and not a tax supported public service. The fire board needs to have the chief add how many calls at $3000 each the LMRFD loses to AMR in the chief's report.
The other day a second ambulance was needed at a traffic accident. The LMRFD ambulance asked AMR to respond from Kingman and AMR refused.
What type of plan does the LMRFD have if local EMS services are overwhelmed like at this accident?
What plan does the LMRFD have to provide EMS services in a major event since only one firefighter/EMT lives in the fire district?
The ambulance needs to be run like a business and not a tax supported public service. The fire board needs to have the chief add how many calls at $3000 each the LMRFD loses to AMR in the chief's report.
The other day a second ambulance was needed at a traffic accident. The LMRFD ambulance asked AMR to respond from Kingman and AMR refused.
What type of plan does the LMRFD have if local EMS services are overwhelmed like at this accident?
What plan does the LMRFD have to provide EMS services in a major event since only one firefighter/EMT lives in the fire district?
Saturday, September 29, 2018
The LMRFD ambulance is a Business So Run It Like One
There was a typical ambulance call in Meadview this morning about 8AM. Dispatch paged Rescue 415 the LMRFD ambulance. After several minutes Rescue 415 advised they were in route.
The caller in Meadview must have figured out nobody was at the Meadview station and the ambulance was coming from Dolan Springs because they canceled the ambulance and took the patient by car.
I understand because fire dispatchers refuse to give you an ETA on the ambulance, something firefighters and law enforcement do all the time. It's also something callers like in Meadview who call 911 need to know.
You should be given the ambulances ETA so you can decide if you want to wait 30-45 minutes for the ambulance or drive the patient to the hospital. You can get to kingman in about an hour, or wait 30-45 minutes for the ambulance and still have the hour drive to Kingman.
This is another example of running the ambulance like a service rather than a business and loosing thousands of dollars a day because they don't actively seek volunteers.
Each time the ambulance isn't available because of lack of manpower we the taxpayers loose $2500.
Each time the ambulance isn't available because of lack of manpower and AMR responds from Kingman we the taxpayers loose $2500.
This happens all the time... 5 times is $12,500... Just 5 times a month is $150,000 a year.....
The caller in Meadview must have figured out nobody was at the Meadview station and the ambulance was coming from Dolan Springs because they canceled the ambulance and took the patient by car.
I understand because fire dispatchers refuse to give you an ETA on the ambulance, something firefighters and law enforcement do all the time. It's also something callers like in Meadview who call 911 need to know.
You should be given the ambulances ETA so you can decide if you want to wait 30-45 minutes for the ambulance or drive the patient to the hospital. You can get to kingman in about an hour, or wait 30-45 minutes for the ambulance and still have the hour drive to Kingman.
This is another example of running the ambulance like a service rather than a business and loosing thousands of dollars a day because they don't actively seek volunteers.
Each time the ambulance isn't available because of lack of manpower we the taxpayers loose $2500.
Each time the ambulance isn't available because of lack of manpower and AMR responds from Kingman we the taxpayers loose $2500.
This happens all the time... 5 times is $12,500... Just 5 times a month is $150,000 a year.....
Friday, September 21, 2018
The Good Old Days When the Fire Station was the Center of Small Communities
Today, most people have never had the need to call the fire department for a fire or EMS and most people don't personally know any firefighters.
The lack of good information many people have about their own fire departments is a big problem especially in underserved areas.
The lack of good information many people have about their own fire departments is a big problem especially in underserved areas.
The LMRFD needs to reach out to the community, teach CPR. Teaching CPR/AED and first aid for free. Help people in this medically underserved area to learn skills to assist the firefighters.
People who participate in training at the local fire department usually come away with a greater appreciation of their firefighters and can become huge allies in future efforts to improve service
Explorer and volunteer programs are a great way to get teenagers, young adults, and even old folks involved in community service. These programs provide greater opportunities for local people to become involved with their fire department they're often great recruiting tools.
The fire station used to be where the guys hung out in small communities. Most were volunteer firefighters and others just friends who stopped by. The fire station doors were usually open and the firefighters friendly and inviting. The few times I've stopped by the fire station in Dolan when someone does crack the door open they look out like what do you want. Monday, July 16, 2018
NACFD1 Petition Signing
NACFD1 Petition Signing
For those interested in helping your local fire district, the Friends of the Northern Arizona Consolidated FD #1 will be circulating petitions for the following:
If you are concerned about the continuing diminished services in Valle Vista, Truxton, Valentine, Chloride and along Stockton Hill Road North of Kingman, please consider signing our petitions.
We will be at the following locations:
- Recall of current directors Mike Collins and Jim Bailey
- Election of former Valle Vista FD Battalion Chief Gerald Lucero as Director in the November election
- Election of former NACFD1 Director Sue Wilkin in the November election
If you are concerned about the continuing diminished services in Valle Vista, Truxton, Valentine, Chloride and along Stockton Hill Road North of Kingman, please consider signing our petitions.
We will be at the following locations:
- 7/16/18 600 PM Valle Vista Propery Owners Association Monthly Meeting (Before and after meeting at clubhouse)
- 7/25/18 400 - 700 PM 2143 Northern Ave. Kingman, AZ (Next to the old smoke shop)
Sunday, July 1, 2018
LMRFD Drug Policy and Volunteers.. Need Your Opinion
I've brought the problem with the LMRFD application and the districts drug policy before. Now I need your opinions..
This is what the LMRFD Drug Policy says......

The policy says "The District prohibits the use, sale, transfer, being under the influence and/or reporting to work after using illicit drugs"
As I read the part that says "Under District policy, alcohol is included within the meaning and prohibition of drugs".
I understand this to say it includes alcohol the same as illicit drugs and employees can't use, sell, transfer, or be under the influence of drugs or alcohol off duty or on duty.
MY QUESTION
If alcohol is included within the meaning and prohibition of drugs, can employees drink alcohol off duty?
I you read this the way I do then employees or volunteers can't even have a beer on the 4th of July.
So why would anyone volunteer, and why are current employees allowed to disregard the drug policy?
How hard is it to change the wording to be more understandable.
ALSO
Please it's obvious you just copied the NACFD application but at least take out the wording that says you're applying for Northern Arizona Consolidated Fire District and not Lake Mohave Ranchos Fire District
LMRFD Application July 1st 2018

This is what the LMRFD Drug Policy says......
The policy says "The District prohibits the use, sale, transfer, being under the influence and/or reporting to work after using illicit drugs"
As I read the part that says "Under District policy, alcohol is included within the meaning and prohibition of drugs".
I understand this to say it includes alcohol the same as illicit drugs and employees can't use, sell, transfer, or be under the influence of drugs or alcohol off duty or on duty.
MY QUESTION
If alcohol is included within the meaning and prohibition of drugs, can employees drink alcohol off duty?
I you read this the way I do then employees or volunteers can't even have a beer on the 4th of July.
So why would anyone volunteer, and why are current employees allowed to disregard the drug policy?
How hard is it to change the wording to be more understandable.
ALSO
Please it's obvious you just copied the NACFD application but at least take out the wording that says you're applying for Northern Arizona Consolidated Fire District and not Lake Mohave Ranchos Fire District
LMRFD Application July 1st 2018

Sunday, June 24, 2018
Does the LMRFD Look for Full Time Firefighters, or is the Good Ol' Boy system alive and well in the LMRFD.
The majority of LMRFD firefighters only work part for the LMRFD while living and working full time for other fire districts in the area.
So why doesn't the LMRFD advertise for full time firefighter EMT's or paramedics? Every time I ask why the LMRFD doesn't hire full time firefighters, I'm told no firefighters want to work here.
But wait all the chiefs buddies work here? Rather than look for full time employees Chief DeMaio hires his buddies from neighboring fire districts. Paramedics make almost $700 per shift plus benefits and retirement costs. They work 2 days at their fire district, 2 days at LMRFD and still get 2 days off...
So rather than look for full time firefighters who want to live in the fire district, it appears the Good Ol' Boy system is alive and well in the LMRFD.
Young firefighter EMT's want to use their skills, not sit around. In states like Washington where fire departments are under civil service a young firefighter wanting to work for Spokane Fire Department will take the civil service test. Then wait to see where they are on the hiring list that will be used for the next two years, if there are any openings.
Even young firefighter's who placed high on the list that want to work now had better look somewhere else to work until a job at Spokane Fire Department opens up sometime in the next two years.
I know in 2015 LMRFD paramedics were making $13.98 an hour, or $669.69 per 48 hour shift, or $2678 a month plus benefits of approximately $800 a month. Thats working 10-11 days a month with 19-20 days off a month.
We live in a place where people bring their ATV's, 4X4's and other toys to play. We have good weather all year, compared to being ass deep in snow up north.
You can't tell me if the LMRFD would advertise at firefighting schools nation wide, that young firefighters wouldn't come here to work 10 days a month for $3500 (with benefits) a month, and play with their toys the other 20 days.
The LMRFD needs to advertise at fire schools nation wide, like other fire districts.
So why doesn't the LMRFD advertise for full time firefighter EMT's or paramedics? Every time I ask why the LMRFD doesn't hire full time firefighters, I'm told no firefighters want to work here.
But wait all the chiefs buddies work here? Rather than look for full time employees Chief DeMaio hires his buddies from neighboring fire districts. Paramedics make almost $700 per shift plus benefits and retirement costs. They work 2 days at their fire district, 2 days at LMRFD and still get 2 days off...
So rather than look for full time firefighters who want to live in the fire district, it appears the Good Ol' Boy system is alive and well in the LMRFD.
Young firefighter EMT's want to use their skills, not sit around. In states like Washington where fire departments are under civil service a young firefighter wanting to work for Spokane Fire Department will take the civil service test. Then wait to see where they are on the hiring list that will be used for the next two years, if there are any openings.
Even young firefighter's who placed high on the list that want to work now had better look somewhere else to work until a job at Spokane Fire Department opens up sometime in the next two years.
I know in 2015 LMRFD paramedics were making $13.98 an hour, or $669.69 per 48 hour shift, or $2678 a month plus benefits of approximately $800 a month. Thats working 10-11 days a month with 19-20 days off a month.
We live in a place where people bring their ATV's, 4X4's and other toys to play. We have good weather all year, compared to being ass deep in snow up north.
You can't tell me if the LMRFD would advertise at firefighting schools nation wide, that young firefighters wouldn't come here to work 10 days a month for $3500 (with benefits) a month, and play with their toys the other 20 days.
The LMRFD needs to advertise at fire schools nation wide, like other fire districts.
Sunday, June 17, 2018
Common Sense? What Does Common Sense Tell You About this Picture?
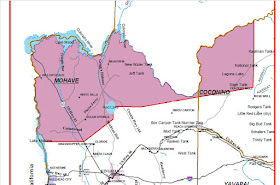
They say a picture is worth 1000 words. I hope this image of all the fire districts in Mohave County and the LMRFD CON does this for you..
The brown line outlines Mohave County. The blue square in the red line is the Dolan portion of the LMRFD. The two little blue spots just above are the Meadview portion of the LMRFD.
The red line is approximately the 2200 square miles in the LMRFD CON.

The brown line outlines Mohave County. The blue square in the red line is the Dolan portion of the LMRFD. The two little blue spots just above are the Meadview portion of the LMRFD.
The red line is approximately the 2200 square miles in the LMRFD CON.

As you can see the LMRFD is much larger than most of the other fire districts in the county. The CON or ambulance coverage area area covered by our 2-3 firefighters is larger than all the other fire districts in the county combined.
We need to ask why the taxpayers in the small medically under served communities of Dolan Springs and Meadview support an ambulance that covers an area larger than ALL OTHER FIRE DISTRICTS in Mohave County?
We need to reduce the area of the LMRFD to the area of the fire district. We're told the ambulance needs the money from calls.
The majority of calls are from the populated areas in Dolan and Meadview. How much does the ambulance make, or lose on calls outside the fire district? Does anyone know?
The taxpayers in those two little blue dots on the map can not be expected to support EMS for such a huge area.
Thursday, June 14, 2018
Fire an Example of WHY We Need to Separate the LMRFD Fire Service from Ambulance
I hope other people have a problem with it taking an hour to an ambulance to a call, especially when it's an injured firefighter.
When one of our firefighters suffers heat exhaustion working a fire in 100 degree temperatures and rather than have the volunteer resources to use our NEW $163,000 ambulance, they call for AMR ambulance from Kingman. CORRECTION The Ambulance was $163,000
At yesterdays fire on Ivy one of our firefighter who risk their lives to protect us suffered heat exhaustion fighting the fire. There seemed to be some confusion on the call about if an ambulance was needed.
Around 4 PM LMRFD advised they had a firefighter with heat exhaustion a requested AMR respond from Kingman.
At 4:17 PM LMRFD asked dispatch if AMR was responding, they weren't. Dispatch asked if this was for a transport, and LMRFD told them yes, this was a firefighter with heat exhaustion that needed transport.
At 4:41 LMRFD again checked on AMR telling dispatch that they needed a Delta Response, red lights and siren...
At 4:54 PM AMR finally arrived and the firefighter wasn't finally transported at 5:04 PM.
Something is wrong when we have a $163,000 ambulance is sitting a mile away while a firefighter suffering heat exhaustion. Waiting an hour for an ambulance on any EMS call is just wrong. When one of our firefighters is injured they need to become the priority.
The LMRFD put a volunteer firefighter through the recent EMR Emergency Medical Responder course and should be nationally certified by now.
The LMRFD should be asking the Arizona EMS Bureau why the Arizona Revised Statutes say an EMR can work on an ambulance and assist EMT's and paramedics and drive the ambulance.
AGAIN a two man crew, one EMT and one paramedic can not run a cardiac arrest call and transport. It takes a minimum of 3 preferably 4 people to run a cardiac arrest and do EFFECTIVE CPR on scene or in the ambulance during transport.
When one of our firefighters suffers heat exhaustion working a fire in 100 degree temperatures and rather than have the volunteer resources to use our NEW $163,000 ambulance, they call for AMR ambulance from Kingman. CORRECTION The Ambulance was $163,000
At yesterdays fire on Ivy one of our firefighter who risk their lives to protect us suffered heat exhaustion fighting the fire. There seemed to be some confusion on the call about if an ambulance was needed.
Around 4 PM LMRFD advised they had a firefighter with heat exhaustion a requested AMR respond from Kingman.
At 4:17 PM LMRFD asked dispatch if AMR was responding, they weren't. Dispatch asked if this was for a transport, and LMRFD told them yes, this was a firefighter with heat exhaustion that needed transport.
At 4:41 LMRFD again checked on AMR telling dispatch that they needed a Delta Response, red lights and siren...
At 4:54 PM AMR finally arrived and the firefighter wasn't finally transported at 5:04 PM.
Something is wrong when we have a $163,000 ambulance is sitting a mile away while a firefighter suffering heat exhaustion. Waiting an hour for an ambulance on any EMS call is just wrong. When one of our firefighters is injured they need to become the priority.
The LMRFD put a volunteer firefighter through the recent EMR Emergency Medical Responder course and should be nationally certified by now.
The LMRFD should be asking the Arizona EMS Bureau why the Arizona Revised Statutes say an EMR can work on an ambulance and assist EMT's and paramedics and drive the ambulance.
AGAIN a two man crew, one EMT and one paramedic can not run a cardiac arrest call and transport. It takes a minimum of 3 preferably 4 people to run a cardiac arrest and do EFFECTIVE CPR on scene or in the ambulance during transport.
Friday, June 8, 2018
There is a Difference Where You Train and I Found When You Train... How I've Found EMS Has Changed
I recently completed my 80 hour EMR Emergency Medical Responder training and passed my National Registry of Emergency Medical Technicians test to become a Nationally Registered Emergency Medical Responder.
The training today was certainly different than my training back in 1984. They have had great advances in EMS training, medications and equipment. I noticed things had changed in EMS but there were also drastic changes in the way emergency departments are ran.
I did much of my EMS training at the emergency room at County Hospital in Los Angels. Ya it was way back in 1984 the Olympics were in town as well as millions of extra people from all over the world and it was a crazy time in EMS. Emergency Medicine was in it's beginning and they were starting to train paramedics across the U.S.
NOTE for General Hospital Watchers
Across the street from the County Hospital in Los Angels was the womans hospital. So the main County Hospital building was know as General Hospital. The big gates you see at the beginning of soap opera General Hospital are the entrance to LA County Hospital Emergency Department...
If you have ever had an interest in emergency medicine and how we got from emergency rooms to emergency departments, from family physicians to emergency medicine physicians, and first aiders to paramedics, County Hospital and what was called C-booth was where emergency medicine was born......
One review said: The documentary Code Black is about County Hospital in Los Angeles and the emergency doctors who work there, and the young physicians, physician assistants, and paramedics who train there. It is literally a gut-wrenching portrait of a small square footage of space where we’re told more people have died and been saved than anywhere else in the United States. It’s a 50 by 25 foot section of the County ER called “c-booth.”
The training today was certainly different than my training back in 1984. They have had great advances in EMS training, medications and equipment. I noticed things had changed in EMS but there were also drastic changes in the way emergency departments are ran.
I did much of my EMS training at the emergency room at County Hospital in Los Angels. Ya it was way back in 1984 the Olympics were in town as well as millions of extra people from all over the world and it was a crazy time in EMS. Emergency Medicine was in it's beginning and they were starting to train paramedics across the U.S.
NOTE for General Hospital Watchers
Across the street from the County Hospital in Los Angels was the womans hospital. So the main County Hospital building was know as General Hospital. The big gates you see at the beginning of soap opera General Hospital are the entrance to LA County Hospital Emergency Department...
If you have ever had an interest in emergency medicine and how we got from emergency rooms to emergency departments, from family physicians to emergency medicine physicians, and first aiders to paramedics, County Hospital and what was called C-booth was where emergency medicine was born......
It's sad but today emergency medicine is about privacy,
liability, and paper work, and not medicine....
Code Black shows you the change from saving lives at the Old County Hospital, to doing paper work at the New County Hospital
One review said: The documentary Code Black is about County Hospital in Los Angeles and the emergency doctors who work there, and the young physicians, physician assistants, and paramedics who train there. It is literally a gut-wrenching portrait of a small square footage of space where we’re told more people have died and been saved than anywhere else in the United States. It’s a 50 by 25 foot section of the County ER called “c-booth.”
As crazy as things got on the popular ER drama, that show doesn’t hold a candle to the insanity
that happened at “C-booth,” where the worst trauma cases were taken. The horde
of doctors and PA’s and EMT’s that surround a dying man looks like what would
happen if you dropped the guy in the middle of a crowded Tokyo train.
If you have Netflix check out Code Black the Documentary
Be Safe Be Prepared Learn CPR and First Aid
Thursday, June 7, 2018
WE have been told over and over that "the LMRFD Certificate of Necessity Can NOT be Changed So WHO CHANGED IT?
WE have been told over and over that "the LMRFD Certificate of Necessity Can NOT be Changed... Period.....
REALLY!!! Then WHO CHANGED IT?
At one time the LMRFD had the resources to cover the 2200 square mile CON or Certificate of Necessity form the state. WHY Can't we change the area covered by the LMRFD Ambulance since our resources have changed from seven ambulances to one.
At one time the LMRFD web page said the fire district had seven ALS (Advanced Life Support) ambulances and four rescue vehicles with extradition equipment...

At the LMRFD board meetings we have been told over and over that the LMRFD CON Certificate of Necessity can NOT be changed. Period... NOT TRUE
The image below is a map of the LMRFD CON Certificate of Necessity issued by the Arizona EMS Bureau.
As you can see the CON covers a huge area that extends into Coconino County. The LMRFD Does NOT RESPOND to calls in the eastern part of the CON or in Coconino County.
In fact, if you look at a map, you can't get there from here....
To get from the LMRFD fire station in Dolan Springs to the eastern part of the CON is on Route 66. From Dolan Springs to Frazier Wells is 116 miles and takes a little over 2 hours to get there... If responding from Meadview it's 133 miles and 2 1/2 hours to get there.
We need to ask why if the CON can NOT BE CHANGED, who made this change, is it legal to reduce the CON area without advising the MS Board.
If they reduced the CON in this case, why can't we reduce the CON to cover the 144 square mile fire district. If people in White Hills want fire and ambulance service join the fire district and pay their fair share or start their own fire district and ambulance.
Currently the taxpayers in the 144 sm LMRFD are the only one's supporting the basic fire and EMS services. Yes people in White Hills pay when they call the ambulance.
I question how much the LMRFD has recovered responding to fires outside the district like the fire at Rosie's Den and others.
How much do we get is kind of a moot point if our only firefighters are up in White Hills when your home burns down or your husband dies of a heart attack.
Why don't the taxpayers in the LMRFD get it? Why is the LMRFD Ambulance the ONLY fire ambulance that covers 2000 square miles OUTSIDE their fire district.
If we had seven ALS (Advanced Life Support) ambulances and four rescue vehicles with extradition equipment and volunteers around the fire district, we could cover 2200 sm's...
BUT we don't, we have one ambulance...
We have a broken EMS service in the LMRFD and it needs fixed....
REALLY!!! Then WHO CHANGED IT?
At one time the LMRFD had the resources to cover the 2200 square mile CON or Certificate of Necessity form the state. WHY Can't we change the area covered by the LMRFD Ambulance since our resources have changed from seven ambulances to one.
At one time the LMRFD web page said the fire district had seven ALS (Advanced Life Support) ambulances and four rescue vehicles with extradition equipment...

At the LMRFD board meetings we have been told over and over that the LMRFD CON Certificate of Necessity can NOT be changed. Period... NOT TRUE
The image below is a map of the LMRFD CON Certificate of Necessity issued by the Arizona EMS Bureau.
As you can see the CON covers a huge area that extends into Coconino County. The LMRFD Does NOT RESPOND to calls in the eastern part of the CON or in Coconino County.
In fact, if you look at a map, you can't get there from here....
To get from the LMRFD fire station in Dolan Springs to the eastern part of the CON is on Route 66. From Dolan Springs to Frazier Wells is 116 miles and takes a little over 2 hours to get there... If responding from Meadview it's 133 miles and 2 1/2 hours to get there.

We need to ask why if the CON can NOT BE CHANGED, who made this change, is it legal to reduce the CON area without advising the MS Board.
If they reduced the CON in this case, why can't we reduce the CON to cover the 144 square mile fire district. If people in White Hills want fire and ambulance service join the fire district and pay their fair share or start their own fire district and ambulance.
Currently the taxpayers in the 144 sm LMRFD are the only one's supporting the basic fire and EMS services. Yes people in White Hills pay when they call the ambulance.
I question how much the LMRFD has recovered responding to fires outside the district like the fire at Rosie's Den and others.
How much do we get is kind of a moot point if our only firefighters are up in White Hills when your home burns down or your husband dies of a heart attack.
Why don't the taxpayers in the LMRFD get it? Why is the LMRFD Ambulance the ONLY fire ambulance that covers 2000 square miles OUTSIDE their fire district.
If we had seven ALS (Advanced Life Support) ambulances and four rescue vehicles with extradition equipment and volunteers around the fire district, we could cover 2200 sm's...
BUT we don't, we have one ambulance...
We have a broken EMS service in the LMRFD and it needs fixed....
Tuesday, May 29, 2018
Volunteer Firefighters a Need NOT a Want for Rural Fire Districts
NFPA estimates there were approximately 1,160,450 local firefighters in the U.S. in 2015. Of the total number of firefighters 345,600 (30%) were career firefighters and 814,850 (70%) were volunteer firefighters. Volunteer firefighters are the key to fire service and EMS in smaller
In the LMRFD recruiting volunteers is not the priority, recruiting full time firefighters isn't the priority either. I've never seen an advertisement for volunteers or any recruiting from fire and EMS training schools like other districts.
I was sad to see Chief Eder leave the NACFD. Chief Eder was more proactive about training and firefighter safety than other chiefs, especially for the volunteers. Chief Eder was a volunteer firefighter, his father was volunteer firefighter, and his grandfather was a volunteer firefighter.
He saw the value of volunteers who not only saved the district money, they provided manpower when needed providing additional support and safety for firefighters. In rural fire districts manpower is the most important factor. When an RV exploded in fire causing a womans death in the LMRFD, one firefighter showed up.
Nation wide 7 out of 10 firefighters are volunteers. This is especially true in smaller communities like Dolan Springs, Chloride, White Hills, and Meadview. I'm afraid nothing will change in the LMRFD until we have a different fire chief. A chief who understands the majority of calls are EMS and the need for volunteer first responders to be trained in EMS and not required to be a firefighter.
In the city firefighters have several things on their side, support services, response times, hydrants for water supply, and manpower. In rural fire districts response times are long and water is supplied by water tenders, formerly called tankers. It takes time equipment and manpower to move thousands of gallons of water to the fire.
What training did your fire district provide their volunteers?
This is my training provided by NACFD since September 2017...
Standard First Aid/CPR/AED
Nationally Certified Emergency
Medical Responder
Wildland Fire Orientation
S-110 Basic Wildland Fire Orientation
Incident Command System I-100
National Incident Management
System N-700
Hazardous Materials First
Responder-Operations
Hazardous Materials First
Responder-Awareness
S-130 Firefighter Training Classroom
S-130 Firefighter Training Field/Practical
Type 6 Engine Operations
Exterior Structural Firefighting
District Orientation/Safety
EVOC Emergency Vehicle Operation
Incident Rehab 2 Water Tender
Operations
Emergency Communications
If you live in the NACFD Check Out Friends of NACFD #1 Blog
Sunday, May 27, 2018
Follow Up on December 2016 Fatal Accident You Decide Cover UP?
On December 22nd 2016 there was a fatal accident on US-93 where an 18 year old boy was left to die. This is my ORIGINAL POST about the December 22nd 2016 fatal accident
I have been around EMS all my life. I've seen ambulances diverted to more serious patients numerous times. I have NEVER seen an ambulance diverted from a critical patient to a non-critical patient with a broken bone.
This is the heavily redacted EMS Bureaus REPORT on a complaint I filed against the LMRFD. I've seen redacted documents before, and understand HIPPA laws, but not only identifiers were removed from this document, all identifiers, locations, and many times were redacted. WHY this isn't some secret military operation requiring times and locations to be redacted, it's an accident on a US highway.
This is my ORIGINAL COMPLAINT to the EMS Bureau without redaction
You tell me.... I understand not identifying a patients private information like in the identifiers listed below, name, DOB, address, and account numbers..... BUT when they redact words like him, he, wife, Kingman, locations like mile posts and mile post numbers, and arrival times for EMS.
It looks like someone is covering up something....
These are the HIPAA Identifiers that should be removed from medical documents.
I have been around EMS all my life. I've seen ambulances diverted to more serious patients numerous times. I have NEVER seen an ambulance diverted from a critical patient to a non-critical patient with a broken bone.
This is the heavily redacted EMS Bureaus REPORT on a complaint I filed against the LMRFD. I've seen redacted documents before, and understand HIPPA laws, but not only identifiers were removed from this document, all identifiers, locations, and many times were redacted. WHY this isn't some secret military operation requiring times and locations to be redacted, it's an accident on a US highway.
This is my ORIGINAL COMPLAINT to the EMS Bureau without redaction
You tell me.... I understand not identifying a patients private information like in the identifiers listed below, name, DOB, address, and account numbers..... BUT when they redact words like him, he, wife, Kingman, locations like mile posts and mile post numbers, and arrival times for EMS.
It looks like someone is covering up something....
These are the HIPAA Identifiers that should be removed from medical documents.
HIPAA Safe Harbor standards, 18 identifiers associated with the patient, their household members, relatives and employers must be removed, including:
- Names
- All geographic subdivisions smaller than a state, including street addresses, cities, counties, precincts and ZIP codes
- All elements of dates (except year)
- Telephone numbers
- Fax numbers
- Email addresses
- Social Security numbers
- Medical record numbers
- Health plan beneficiary numbers
- Account numbers
- Certificate or license numbers
- Vehicle identifiers and serial numbers, including license plate numbers
- Device identifiers and serial numbers
- Web URLs
- IP addresses
- Biometric identifiers, including finger and voice prints
- Full-face photographs and any comparable images
- Any other unique identifying number, characteristic or code
Friday, May 25, 2018
My NACFD Resignation
My
NACFD Resignation
I
resign as a volunteer firefighter for the NACFD.
I
was disappointed in Board Chair Jim Bailey’s knowledge of what an EMR or
Emergency medical Responder’s skills were. Saying an EMR was just someone who
took a first aid class.
I did some checking on EMR’s before we started the class at NACFD.
In the Arizona Bureau of EMS Statutes and Rules Book where I found that under
Arizona law “an emergency medical responder is someone who is employed by an
ambulance service” and “whose primary responsibility is the driving of an
ambulance”.
ARS 36-2201
6. "Ambulance
attendant" means any of the following:
(b) An emergency medical responder who is employed by an ambulance service
operating under section 36-2202 and whose primary responsibility is the driving
of an ambulance.
8. "Basic life support" means
the level of assessment and care identified in the scope of practice approved
by the director for the emergency
medical responder and emergency medical technician.
16. "Emergency
medical responder" as an ambulance attendant means a person who has
been trained in an emergency medical responder program certified by the
director or in an equivalent training program and who is certified by the
director to render services pursuant to section 36-2205.
I also
went to the National Registry of Emergency Medical Technicians web page. These
are the people who nationally certify you as an EMR, EMT, or paramedic before
you get certified by your state EMS Bureau.
On the
National Registry of Emergency Medical Technicians Arizona Bureau of EMS page
under EMS License Levels it says Arizona licenses Emergency Medical Responders,
Emergency Medical Technicians, Advanced Emergency Medical Technicians, and
Paramedics. https://www.nremt.org/rwd/public/states/state-ems-agencies/az
So unless someone actually called the Arizona EMS
Bureau and asked, “do you certify EMR’s” it says so on the National
Registry of Emergency Medical Technicians web page, and in the ARS, but what do
they know?
I
checked the National EMS Scope of Practice Model at EMS.gov and found there’s
really not a lot of difference between an EMR and a EMT Basic with no
additional training.
NOTE
The Arizona EMS Bureau DOES NOT Recognize EMR’s WHY is
what we need to ask….
I
love when people listen to rumors and BS rather than check for themselves,
especially when it comes to the law. It always makes them look ignorant.
Chairman Bailey EMR’s can do CPR, but yes you were kind of
right about that, but EMR’s do so much more than a first aid person.
EMR’s do need to take the American Heart Association Basic
Life Support CPR and AED program for BLS providers. The very same Basic Life
Support CPR and AED program that EMT’s and Paramedics are required to take.
EMR’s can also use Airway and Breathing Adjuncts including the
insertion of airway adjuncts intended to go into the oropharynx or nasopharynx.
They can use positive pressure ventilation devices such as the bag-valve-mask
to assist in breathing.
When someone’s airway is obstructed with vomit or bone, an EMR
can suction the upper airway, and give supplemental oxygen therapy. And if that
time comes, do CPR and use an automated external defibrillator.
They can do some very limited pharmacological interventions,
manually stabilize suspected cervical spine injuries, do manual stabilization
of extremity fractures, and control bleeding.
Chairman Bailey does that sounds like a basic first aider?
The National Scope of Practice says “A major difference
between the Emergency Medical Responder and the Emergency Medical Technician is
the knowledge and skills necessary to provide medical transportation of
emergency patients”
So they get more training on loading and transporting patients
than an EMR and they can do these additional skills.
1. Airway and Breathing Insertion of airway adjuncts intended to
go into the oropharynx or nasopharynx
2. Use of positive pressure ventilation devices such as manually
triggered ventilators and automatic transport ventilators
3. Assist patients in taking their own prescribed medications
4. Administration of the following over-the-counter medications
with appropriate medical oversight: Oral glucose for suspected hypoglycemia and
aspirin for chest pain of suspected ischemic origin
5. Trauma Care Application and inflation of the pneumatic
anti-shock garment (PASG) for fracture stabilization
So the only difference between an EMR and an EMT Basic with no
additional advanced training is the EMT can:
1. Use a better airway to secure your airway
2. Help you open your own medicine and take it
3. Use an positive pressure ventilation device as opposed to a
bag valve mask
4. They can give over-the-counter medications like glucose (sugar)
or aspirin with appropriate medical
5. In trauma they can use a pneumatic anti-shock garment what we
used to call MAST Pants.
6. Has the training to load and transport a patient by ambulance.
It’s sad when people who oversee vital services like the fire
service understand so little about what firefighters and EMS providers do, and
their levels of training.
Thank you for allowing me to train with
the firefighters of NACFD
Jay Fleming
Dolan Springs AZ
LINK to Chief Eder's Blog
Wednesday, May 9, 2018
Why Does the LMRFD Make It So Difficult to Read the Fire Board Minutes?
I must not be the only person who feels frustrated reading the fire board minutes.
Does the LMRFD make it difficult to read the fire board minutes on purpose? It's so hard to read because you need to scroll up and down, then use the little arrow to move to additional pages, then scroll up and down.
They lock the text so you can't cut and past text. Why not use a format where citizens can read the entire minutes or even save or print a copy?
Why not start a Facebook page like the Kingman Fire Department https://www.facebook.com/KingmanFire or Bullhead City Fire https://www.facebook.com/bullheadcityfd or Mohave Valley Fire https://www.facebook.com/Mohave-Valley-Fire-Department-405362549662347
Or the hundred other fire districts and departments. The LMRFD needs to be more citizen friendly when it comes to providing citizens information..
Does the LMRFD make it difficult to read the fire board minutes on purpose? It's so hard to read because you need to scroll up and down, then use the little arrow to move to additional pages, then scroll up and down.
They lock the text so you can't cut and past text. Why not use a format where citizens can read the entire minutes or even save or print a copy?
Why not start a Facebook page like the Kingman Fire Department https://www.facebook.com/KingmanFire or Bullhead City Fire https://www.facebook.com/bullheadcityfd or Mohave Valley Fire https://www.facebook.com/Mohave-Valley-Fire-Department-405362549662347
Or the hundred other fire districts and departments. The LMRFD needs to be more citizen friendly when it comes to providing citizens information..
Monday, April 16, 2018
When the hospital is a half hour away and it's shift change a helicopter may sound like a great option
Medical Helicopter transports can be a life saving tool in the right circumstances. It can and has been a death sentence for the wrong patient.
A couple weeks ago around 6 AM there was a cardiac arrest call on Maywood Dr, about 3 miles from the LMRFD fire station in Dolan Springs. The LMRFD ambulance responded and when on scene called for a medical helicopter to respond to the Dolan Springs fire station. They were told the helicopter would have a 21 minute ETA once launched.
The LMRFD ambulance sat at the fire station for over 20 minutes before canceling the medical helicopter and transporting the patient to KRMC.
THE AGE-OLD DEBATE ON EMS HELICOPTER USE
A IS FOR ACCESS
L IS FOR LAZY
T IS FOR TIME
E IS FOR EXTRICATION
R IS FOR REAL
FLYING TAKES TIME
A couple weeks ago around 6 AM there was a cardiac arrest call on Maywood Dr, about 3 miles from the LMRFD fire station in Dolan Springs. The LMRFD ambulance responded and when on scene called for a medical helicopter to respond to the Dolan Springs fire station. They were told the helicopter would have a 21 minute ETA once launched.
The LMRFD ambulance sat at the fire station for over 20 minutes before canceling the medical helicopter and transporting the patient to KRMC.
My problem is it's 30-35 minutes from Dolan Springs to KRMC Emergency Room. The Air Ship takes 10-15 minutes for the air crew to be alerted, respond and do their preflight checks and take off. Flight time to scene, in this case 21 minutes after launch.
We have no protocols telling EMS personal when to call for a medical helicopter here. We have a you-call we-haul policy on $25,000 medical helicopter transport.
Preflight routine takes time. Rapid pre-flight shortcuts have been cited in several recent air ambulance crashes.
Once in the air, we need to add in the actual flight time to the scene. If the wind is blowing, the helicopters transit time may be considerably longer in one direction that the other. Once over the scene, the crew will need to assess the safety of the landing zone prior to landing.
Once they have landed, the pilot may require certain criteria before the crew can disembark (especially if the ground is not level). The crew may need to sit on scene and wait to exit the aircraft. Then, the crew will need to receive a hand-off report and package the patient. Based on the crew’s policies, they may also need to perform procedures (like RSI) prior to loading the patient. Space is limited inside the aircraft, so some procedures may need to be completed on the ground.
They will then take off again, fly back to the hospital, land the aircraft, wait to disembark again, transfer the patient into the hospital (sometimes using a second ambulance or a rooftop elevator) and hand off the patient to the staff.
Even in ideal situations, helicopter transport can take much longer to accomplish than you might expect. It is rarely quicker to fly a patient than it is to load them in your rig and transport them to the hospital.
EMS1 Article: How to Decide When to Call an Air Ambulance
EMS1 Article: How to Decide When to Call an Air Ambulance
Remember the FALTER acronym to make sure you call for a
helicopter transport when time really counts
In 2013, a story hit the news about two children who were flown by
helicopter to a trauma center for minor injuries over the protests of their
parents. The story ignited a new firestorm of debate in the EMS blogosphere as
well as the local newspaper. Opinions ranged from “Suck it up and pay the bill”
to “That’s child abduction!”
From the first-hand reports of the responders, parents and flight
crew, the consensus was that these children didn’t need to be flown to the
hospital. I share that opinion. I also think the story points to a larger
concern. That concern is the frequent misuse of helicopters in EMS care.
THE AGE-OLD DEBATE ON EMS HELICOPTER USE
The subject of helicopter misuse may ring familiar in your
ears. Haven’t we addressed this before?
Indeed we have. Helicopter misuse is a garden-weed issue. It rears
its ugly head over and over again. Each time that the level heads in EMS
education step up and pull the weed, it disappears briefly, only to reemerge
again.
There are times when helicopter transport may benefit your
patient. It’s up to you to decide when it’s time to fly the bird. The question
is, are you using a logical reason for transporting your patient by air?
Let me take a shot at this seemingly never-ending issue with a
brand-new acronym: F.A.L.T.E.R. This is a tool that you can use to remember the
important considerations when deciding if helicopter transport is an
appropriate option for your patient.
F IS FOR FEAR
Ask yourself, am I
making this decision because I’m afraid to spend the next thirty minutes
managing this patient in the back of my medic unit? Would I prefer to hand the
patient off as soon as possible? Though we are loath to admit it, many times we
call the helicopter because we’re scared.
We don’t feel adequate
to manage the patient. The helicopter is our panic button.
Fear is never a reason
to call for alternate transport. Overcome it, load the patient and transport.
Bring additional help if you feel like
A IS FOR ACCESS
Does your scene lend itself to convenient helicopter access? If
not, you may waste minutes or hours trying to move the patient to an acceptable
landing site, or waiting for weather to clear. Bad weather and dicey landing
zones make helicopter operations high-risk endeavors. You are often better off
loading the patient and heading for the hospital. No landing zone, no
helicopter.
L IS FOR LAZY
Much like the fear factor, the laziness element requires a good,
honest gut-check. That requires a high degree of self-perception and honesty.
When the hospital is an hour away and your shift change is twenty minutes away,
a helicopter may sound like a great option.
Helicopters allow us to dodge the time and the work of emergency
transport. We can do the fun skills, hand off the patient on scene, restock the
kit and go home. Sometimes we aren't even required to do our standard
documentation if the patient was handed off to a local air crew.
Helicopters aren't a convenient dodge for doing the hard work of
EMS. If your real motivation for calling the helicopter is because you’d rather
not do the work, you may need to do some personal soul searching. Don't saddle
your patient with a $7,000 or more transport bill. Load the patient and
transport. (MY NOTE $25,000 from Dolan)
T IS FOR TIME
Is time really a factor for your patient? This is a huge question
that we can’t just conveniently overlook. There are very few clinical
emergencies that are proven to benefit from reduced time to definitive care.
Significant trauma, strokes and myocardial infarction may all
benefit from a reduced transport time. Diabetic emergencies, minor injuries and
stable patients with scary-looking mechanisms of injury do not benefit from
decreased transport times. (And the first person to say, “What if…” gets a poke
in the eye with a fence post.)
Don’t call the helicopter if you can't assure that the possible
time saved will make a difference in outcome. Use your evaluation skills. If
the patient doesn’t stand to benefit from rapid transport, load the patient and
go.
I don’t want to hear a word about potential rapid decompensation.
The diagnosis needs to support rapid transport right now, period. And the use
of the helicopter has to actually accomplish that goal (see “R is for Real,”
below).
E IS FOR EXTRICATION
Does the patient require extended extrication or extraction from
their location? If the patient meets the requirements for rapid transport, but
is in a situation where their transport will be delayed, consider helicopter
transport. This is one situation where having a helicopter waiting for the
patient might be beneficial. Let’s call it the “sick and stuck” rule. If the
patient is sick and they are stuck, consider calling a helicopter.
For example, if the patient is stuck under their dashboard, pale,
cool and diaphoretic, with a rapid pulse and questionable blood pressure,
consider calling a helicopter. Keep in mind that in most urban areas, a ground
ambulance will still beat the helicopter to the hospital even if the air crew
is waiting on scene for the patient.
R IS FOR REAL
When we consider the helicopter as an alternative to ground
transportation, we have to consider the real time required for helicopter
transport. This is probably the single biggest mistake we make when considering
the appropriateness of helicopter transport. Consider this concept: Helicopter
transport is often very slow.
Here's an example. Calculate your estimated ambulance transport
time, from the point of loading the patient onto your gurney to the point of
making contact with staff at the emergency department.
Now, calculate the time it takes to notify the helicopter crew,
the time it takes for them to scramble the unit, go through their preflight
routine and lift off, and their flight time to the scene.
Then add in the time it takes to land, power down the aircraft,
disembark and receive your patient. Once transferred, they prepare the
patient for flight, clear to take off, fly to the destination, land and
transfer the patient.
Sounds like a lot of steps — and that's true. But let's take a
closer look at some of the steps.
FLYING TAKES TIME
The crew’s preflight routine takes time. Rapid pre-flight
shortcuts have been cited in several recent air ambulance crashes.
Once in the air, we need to add in the actual flight time to the
scene. If the wind is blowing, the helicopters transit time may be considerably
longer in one direction that the other. Once over the scene, the crew will need
to assess the safety of the landing zone prior to landing.
Once they have landed, the pilot may require certain criteria
before the crew can disembark (especially if the ground is not level). The crew
may need to sit on scene and wait to exit the aircraft. Then, the crew will
need to receive a hand-off report and package the patient. Based on the crew’s
policies, they may also need to perform procedures (like RSI) prior to loading
the patient. Space is limited inside the aircraft, so some procedures may
need to be completed on the ground.
They will then take off again, fly back to the hospital, land the
aircraft, wait to disembark again, transfer the patient into the hospital
(sometimes using a second ambulance or a rooftop elevator) and hand off the
patient to the staff.
Even in ideal situations, helicopter transport can take much
longer to accomplish than you might expect. It is rarely quicker to fly a
patient than it is to load them in your rig and transport them to the hospital.
Learn how much time it really takes for a helicopter to fly to
your scene and transport a patient back to the hospital. When you’re selling
the benefits of a helicopter to your patient (or their parents), make sure you consider the real risks, the real benefits and
the real reduction in transport time.
My guess is that the children in that Kentucky store who were
transported in the helicopter might have actually gotten to the hospital faster
if the medic had simply evaluated their wounds, loaded the children and
transported. It would have required more time and more paperwork, but he would
have avoided finding himself on the pages of his local newspaper and various
high-profile EMS blogs.
When you consider calling the helicopter, think realistically.
Evaluate the patient. Be honest with yourself and never FALTER.